
To ORS or not to ORS?
 Shreya Pujari
Shreya Pujari
Countries across the world have been facing increased temperature coupled with rising frequency and intensity of heat waves. Heat is often associated with an array of physiological impacts including heatstroke, dizziness, dehydration and in severe cases, even death. Among these, dehydration has been associated with all age groups with higher vulnerability among infants, younger children and the elderly. It is one of the most commonly observed Heat Related Illness (HRI), which gets further exacerbated due to other converging symptoms of HRIs such as nausea and excessive sweating. One of the most revolutionary measures used to bring downinfant deaths due to dehydration (from diarrhea) back in the 1970s, the Oral Rehydration Solution (ORS), became one of the most recommended solutions to prevent dehydration due to excessive heat. ORS has been widely recognized as a major breakthrough in global health. Within the Indian public health system, ORS is recommended to be made available at all levels, from community health workers to hospitals. In terms of HRIs, while dehydration is often assessed based on urine colour or volume, a robust test to detect the electrolyte fluctuation is not available. Consumption of water quenches thirst and provides relief to a dehydrated body but it may not help to retain that water during excessive heat. A solution like ORS helps to replenish fluids and electrolytes lost due to sweating by helping the body absorb fluids more efficiently, thereby balancing the electrolyte levels and restoring the natural equilibrium of the body. A study by Ishikawa et al. (20101) highlighted that intake of ORS during outdoor work in a hot environment is effective for preventing industrial accidents and heat stroke. While ORS is highly recommended for managing dehydration, there is limited discussion around the need for practicing caution before its intake among specific population groups. Despite its crucial role in the management of dehydration, diarrhea and related malnutrition, serious safety concerns have been raised regarding its use in neonates and young infants. Excessive intake of ORS has been associated with elevated sodium levels (hypernatremia) which can cause seizures, brain damage and even death among infants, swelling (around the eyes and in feet) and excessive irritability while over-dilution of ORS has also been linked to asymptomatic low sodium and potassium levels (hyponatremia and hypokalemia)2. Thus, determining the appropriate concentration of ORS, especially in paediatric use, needs careful consideration.
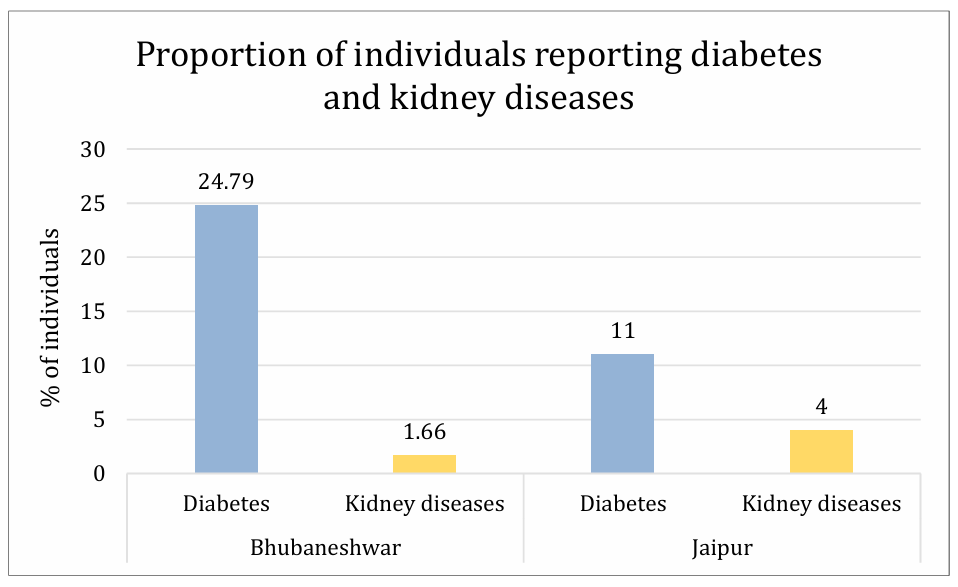
The use of ORS is highly discouraged for people with kidney disorders and those on a fluid-restricted diet. Kidney disorders impair the body’s ability to regulate electrolytes and fluids, so unregulated intake of ORS can increase pressure on the kidneys, which may struggle to manage the extra fluids and electrolyte load (especially sodium and potassium). For patients with chronic diseases such as diabetes, hypertension or heart disease, who are advised to regulate their salt and sugar intake, ORS consumption should be done cautiously. Excessive intake may lead to electrolyte toxicity and disturb the blood sugar or sodium levels in the body. Chronic diseases like diabetes further leads to the development of kidney-related complications. This increased susceptibility also raises concerns regarding the unregulated use of ORS. The Centre for Disease Control and Prevention (CDC) data indicates that approximately 1 in 3 adults with diabetes may develop chronic kidney disease (CKD). The ICMR-INDIAB study (2023) also reported that 40% of people with type 2 diabetes and 30% of those with type 1 diabetes develop kidney diseases. Moreover, death dues to renal failure have been increasing in India, with diabetes being a major contributor3. The primary survey conducted under the CHHANW project in Bhubaneswar, Odisha and Jaipur, Rajasthan reported a substantial proportion of individuals with chronic disease (Diabetes) and kidney diseases, necessitating greater caution in suggesting ORS as a feasible intervention.
So, when a heat intervention is to be put in place, what should be done? To ORS or not to ORS? As the discussions around designing interventions for different vulnerable groups unfolded within the project and consultations with multiple medical professionals were held, it became clear that while ORS is an affordable and accessible measure for dehydration, there is a need for more caution around its consumption, especially when recommended to infants, younger children and elderly. Thus, while ORS remains a life-saving intervention, its administration must be coupled with awareness, especially in India where climate risk and the dual burden of acute and chronic illnesses are simultaneously rising.
For more information, please check: https://chhanw.com/ (Website)
https://www.linkedin.com/company/chhanw/posts/?feedView=all (LinkedIn)
Shreya Pujari
Related Post

Sustainable Cooling Matters
By Sandipta Rath, Anwesha Mishra, Sruti Mohapatra, Purnasha Pany CHHANW team, Institute of Economic Growth “Buying an AC was never a choice but a need. When my father collapsed due to sunstroke during work, we made the decision to prioritize his health even if it means we will be tied to monthly installments and high […]

I am not stronger than heat: Heat-Health Risks Call for Urgent Action from Employers
Summers are getting hotter, and for outdoor workers, the heat isn’t just uncomfortable — it can be dangerous. During my visit to a low-income setting in Jaipur, I met Kishore Kumar (name changed), a 42-year-old construction labourer who learned the hard way how prolonged exposure to extreme heat can take a serious toll — not […]

Where is heat on my priority list?
The intensity and severity of heatwaves in India and across the globe have been steadily rising. Some desert regions in India are now experiencing extreme temperatures—reaching as high as 52°C. What once felt exceptional is now becoming the norm. Every summer, the front pages of newspapers have startling headlines on how heat has broken a […]